
GP Lists & Illegal Migration
What does the patient data tell us about UK migration?

Outline: GP Patient Registrations and Visa Overstays
This paper focuses on the use of our GP surgeries and NHS resources by unauthorised migrants, in particular those who have overstayed their student, visitor, or dependent visas and are, in effect, illegally residing in the UK.
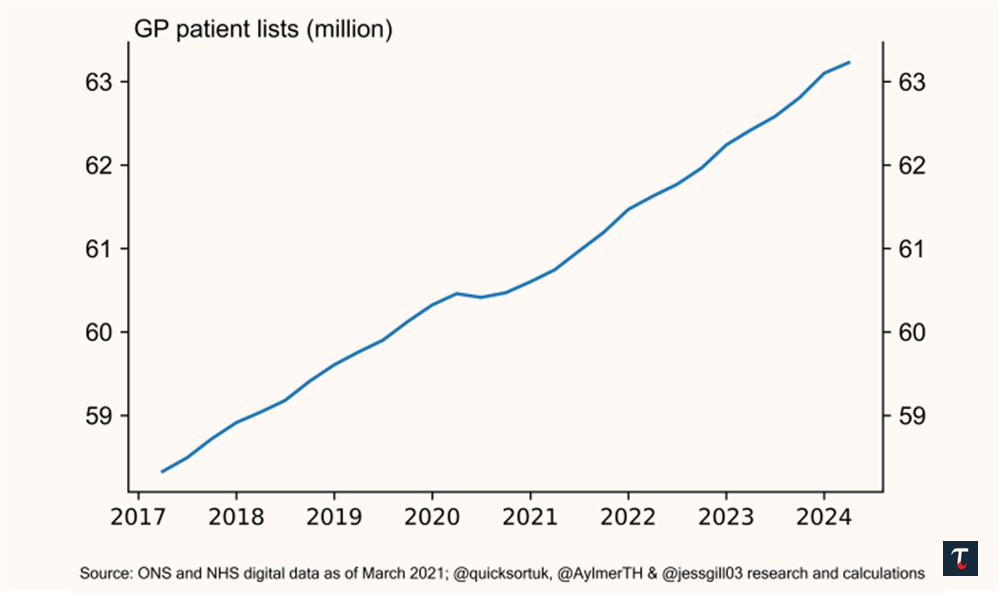
Since 2017, NHS GP patient registrations have increased by five million, see Exhibit 1. Britain’s national debt now approaches 100% of GDP, a 60 year high. These costs are being borne by fewer and fewer people, with the top 1% now paying 28% of the country’s total income tax revenue. This is unsustainable.
When British citizens travel abroad, they are not entitled to free healthcare. Yet since 2018, the NHS has allowed GP practices to remove requirements for a fixed address or any form of ID before registering.1 At present, our NHS can be accessed free at the point of use by unauthorised migrants, neither challenged nor flagged by NHS staff, see Exhibit 2.
How did we get here?
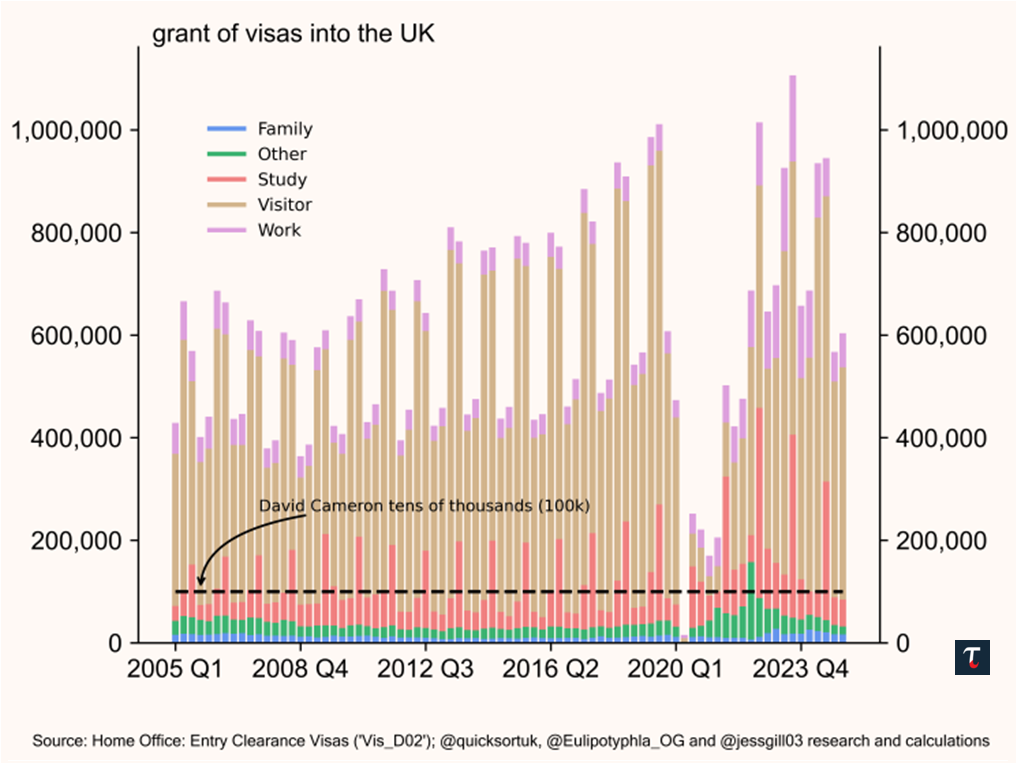
Since 2005, the number of visas issued for work, study, and dependents has hovered around 500,000 to 600,000 per annum. This reached 1.4 million visas per annum under the Boris Johnson Tory Government, not including temporary or visitor visas, see Exhibit 3.
With this scale of migration and lax enforcement, we are interested in visa overstays (both current and historic), and how we can identify these individuals through our existing health system. This paper addresses the following:
I. Where are these illegal migrants typically registered?
II. What is the pattern here?
III. What effective policy changes could be easily made?
IV. What wider changes are required?
V. What mechanisms do we have at our disposal to rectify our healthcare and immigration system?
How many people are staying illegally?
In the latest briefing by Migration Observatory (2025), illegal immigration is categorised in four ways: visa overstays, unauthorised entry, remaining after a failed asylum application, or children born to illegal migrants.2 However, they conclude that there is “limited data to estimate the unauthorised migrant population of the UK”. ²
Pew Research (2019) estimated that there were between 800,000 and 1.2 million illegal migrants in 2017, while the GLA (2020) estimated that there were between 594,000 and 745,000 (and up to 809,000 if including estimates of children born to illegal migrants).² Both used the residual method.
Sajid Javid and Priti Patel asleep at the wheel
In 2019, the Home Office —under Sajid Javid— announced no plans to produce a new residual method study. It added, if they do so in the future, the Ethics Advisory Committee must first decide whether “the access, use and sharing of public data, for research and statistical purposes, is ethical and for the public good”.3 (So, that’s a no then.)
Later, the Home Office —under Priti Patel— announced its exit check statistics had been discontinued since 2020, blaming the “impact of Brexit and the pandemic”.4 Thus for the last five years (2020-25), we do not know the number of visa overstays in the UK. Subsequent Home Secretaries, Suella Braverman, Grant Shapps, and James Cleverly, did not resume this data collection or research either.
Using the 2021 Census Data and GP Lists
Assessing a total of forty-eight million rows of patient list data, we found serious discrepancies between the 2021 census data and 2021 GP patient lists. For a number of areas, we find an excess of patient registrations relative to the number of people recorded in the 2021 Census.
Using Census and Office for National Statistics (ONS) data, we correlated GP locations and patient list characteristics with local area ethnicity for over 30,000 census areas. We identified the following observations:
1. The higher the ethnic minority concentration (under ONS definitions), the greater the excess of registered patients relative to the 2021 Census.
2. This is the case for both the Black British and British Asian communities.
Explaining this trend
One explanation is that there are visa overstays registering or still registered with a GP, while living and working in the UK illegally. Unauthorised migrants often blend into the underground economy, going unnoticed in urban and often ethnically diverse and concentrated communities.
The other explanation is an integration challenge. Lower English proficiency and civic awareness may be reasons why the Census was not completed, leading to discrepancies that occur disproportionately in areas with high concentrations of ethnic minorities.
Both factors are credible, which we endeavour to explore further in this paper.
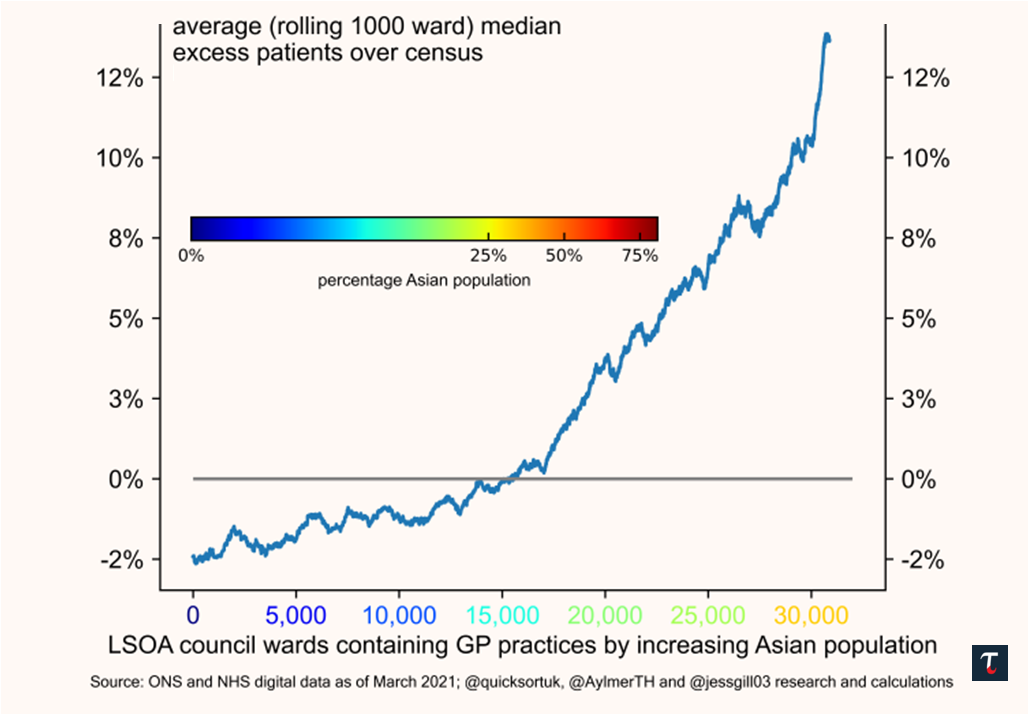
We plot our analysis above, in Exhibit 4. In Chart 4a, all 30,000+ census areas are rank-ordered from least to most Asian concentrated areas, and the average excess registered patients (%) relative to the census data is plotted.
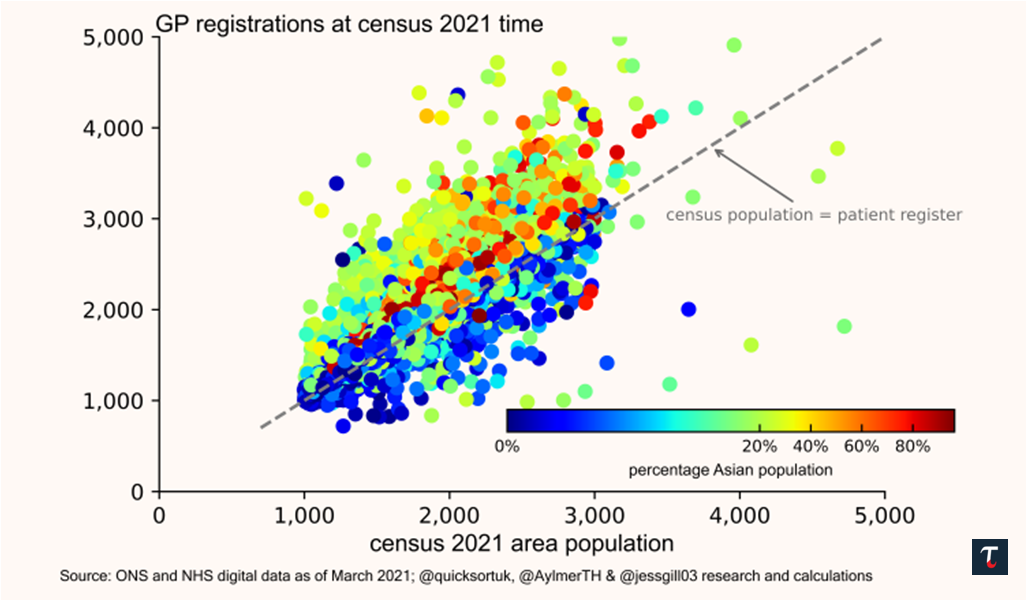
In Chart 4b, we plot census areas by recorded population versus GP patient registrations. Anything above the dashed 1:1 ’parity’ line indicates that GP patient registrations in the area were greater than the population from census data. The colour of each census area indicates the relative British Asian ethnicity of the area, outlined by the colour key.
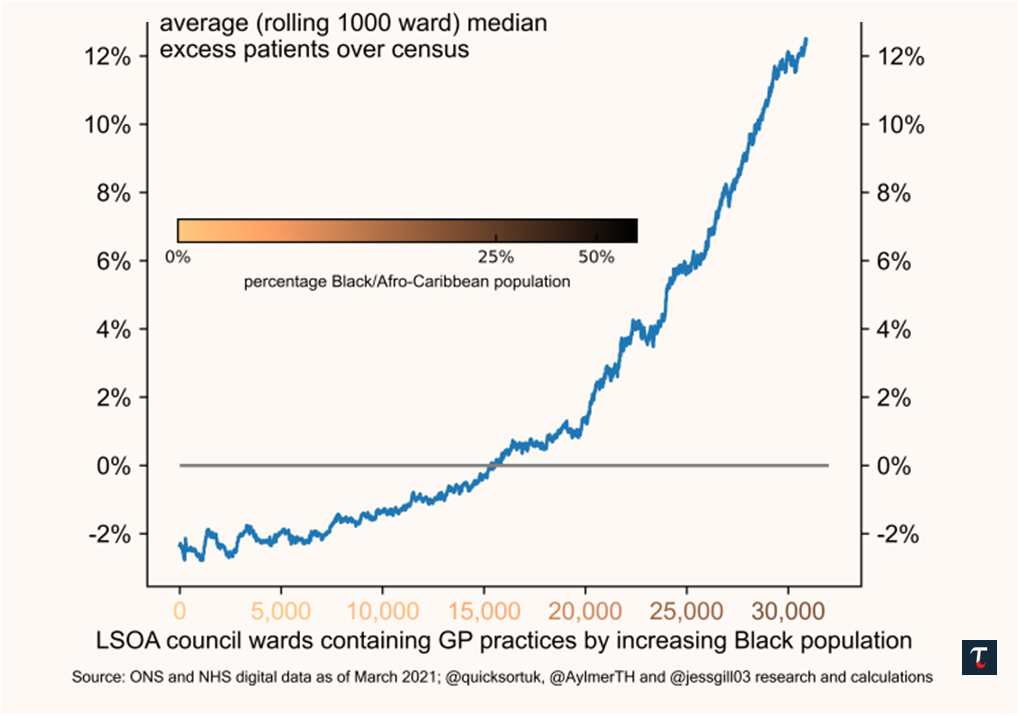
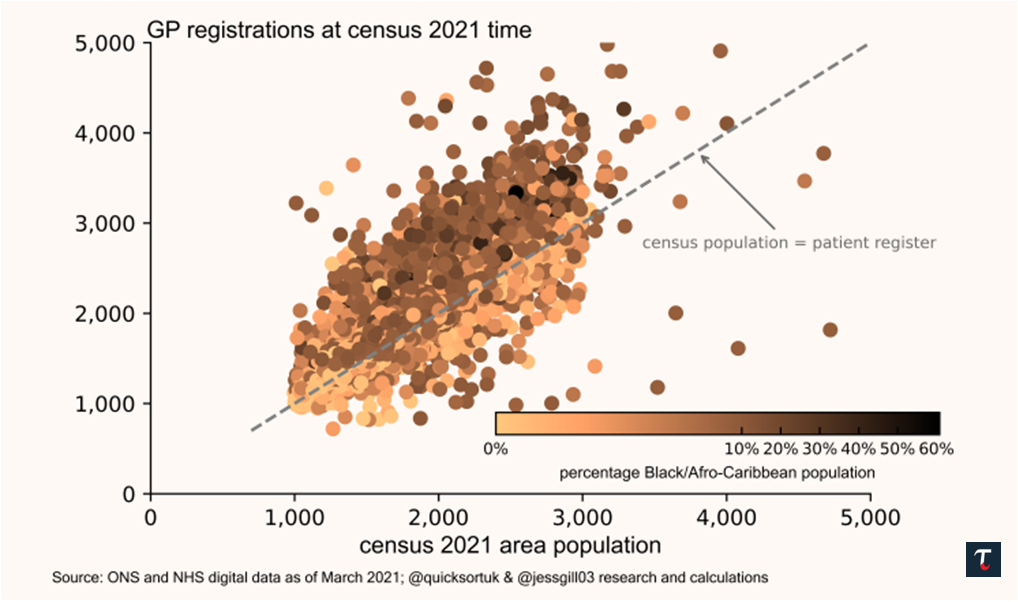
For Exhibit 5, the same process is undertaken for the Black British demographic. In the most concentrated Asian and Black census areas, we find that the patient excess (GP registrations vs census population) is at 10% or greater.
GP Policy Since 2018 and the Third Sector
Since 2018 (principally, after the Homelessness Reduction Act 2017), GP practices have been permitted to forgo basic requirements to verify a patient’s address and identification.5
[Note: The Homelessness Reduction Act 2017 was introduced by Bob Blackman MP, who at the time of writing serves as Chairman of the Parliamentary Conservative Party - the 1922 Committee.]
The charity sector has championed the “Safe Surgeries” open borders policy, with Doctors of the World writing:
“A Safe Surgery can be any GP practice which commits to taking steps to tackle the barriers faced by many migrants in accessing healthcare. At a minimum, this means declaring your practice a ‘Safe Surgery’ for everyone and ensuring that lack of ID or proof of address, immigration status or language are not barriers to patient registration”.
In response to an enquiry, Doctors of the World wrote:
“The guidance also says that even if practices only accept patients in their practice boundary, then patients don’t need to evidence this in the form of official documents, and it isn’t reasonable grounds to refuse registration if the patient is presenting a postcode inside the boundary (or has no fixed address and is registering with the practice address). Although the situation has improved slightly over time... it is still a fairly common issue in many practices across England and a big concern for people who don’t have access to proof of ID and address and are often excluded from accessing primary care.
Our Safe Surgeries network aims to train GP practices to be aware of this guidance and implement changes in practice to ensure their registration policies are inclusive – we have over 2,300 practices signed up at the moment”.
A Matter of Fairness and Resource Choices
“We will keep going until we hit our saturation point, because what does it matter if we have to wait another week for a hospital visit?”, Rachael Maskell MP (video).
While this statement was made by a former Frontbench Labour MP in 2015, since then, the financial or social costs of immigration has not been a political priority for either the Labour or Tory parties. The pretence of compassion across the political spectrum has allowed successive governments to fail to monitor or control visa overstays and illegal migration. Britain does not have infinite resources; facing a rising tax burden, rising National Debt, and stagnant productivity, this state of affairs must come to an end.
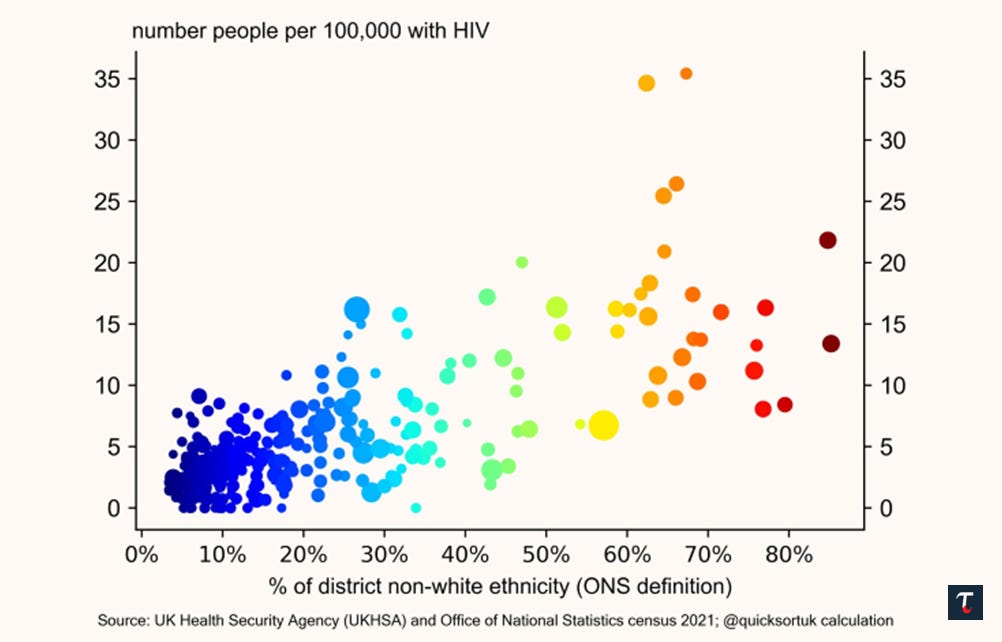
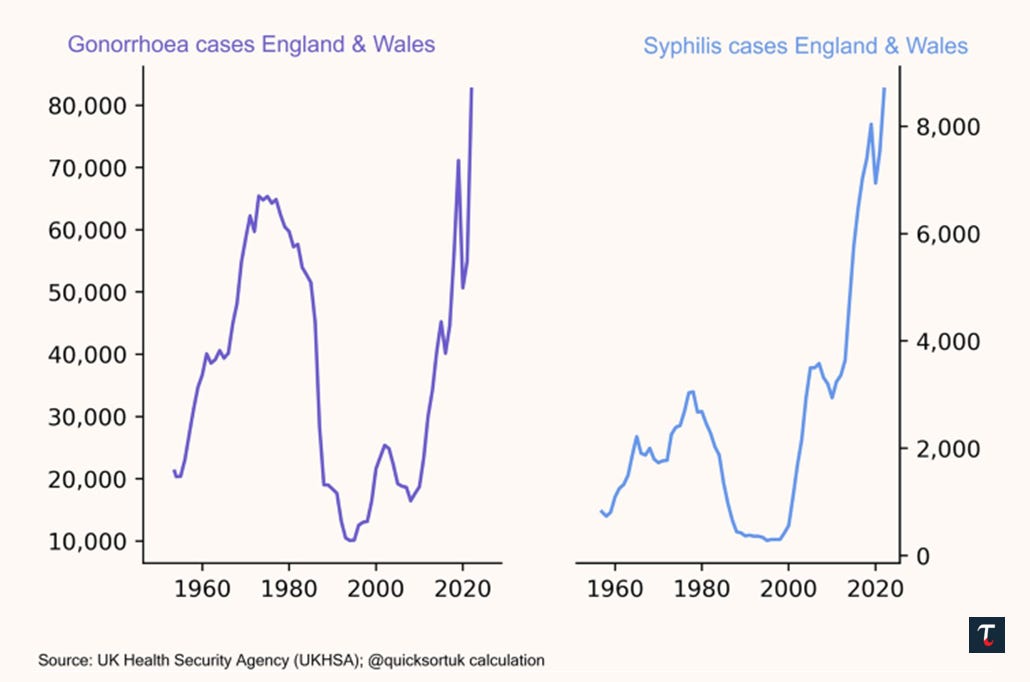
Increased waiting times are not the sole issue either. Immigrant backgrounds have disproportionately higher rates of sexually transmitted diseases, see Exhibits 6 & 7, and Neil O’Brien’s HIV paper.6 This is a real burden on the NHS.
Wider Discussion & Action Points
The link between excess GP patient registrations and heavy first– and second– generation immigrant areas cannot be brushed under the carpet any longer.
NHS policy needs to change. GPs must establish a patient’s right to reside in the UK before registration, and conduct regular checks. There must be a legal obligation to log visa overstays, and other unauthorised migrants.
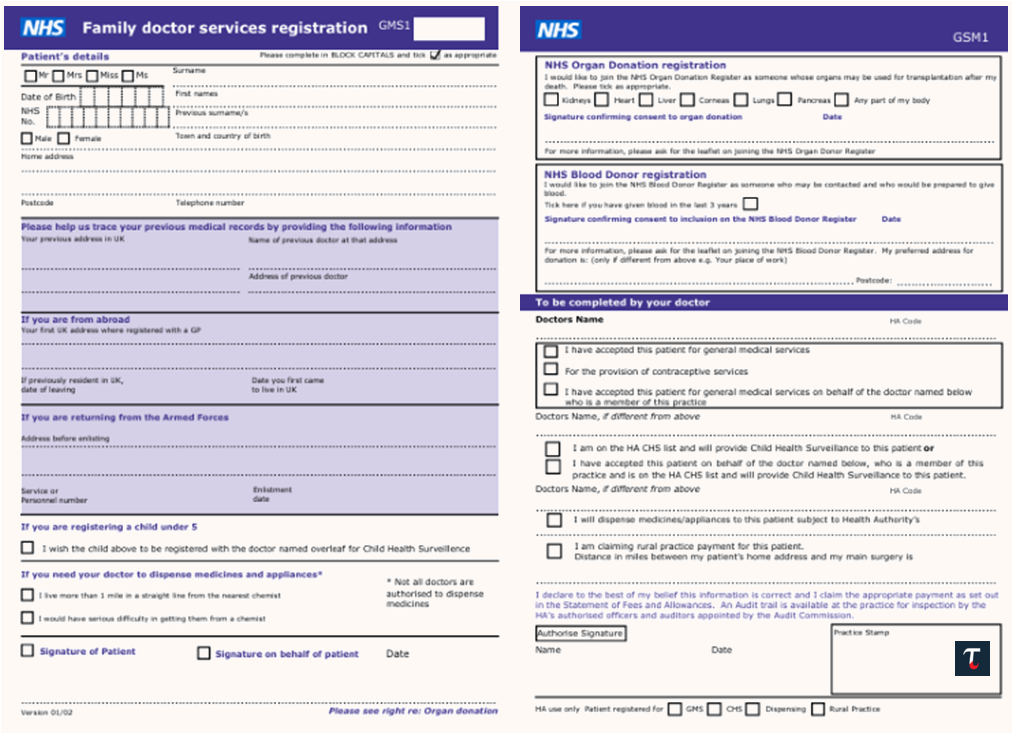
Current GP application forms, known as the ‘purple form’ (see Exhibit 3 earlier), should incorporate passport information, right to residency information, photo ID, and an address as prerequisites to register.
The “Safe Surgeries” policy must end. Amendments to the Health Act 2009 and Homelessness Reduction Act 2017 must follow. GP practices that flout the law and accept third-sector pressure should face heavy fines, and potentially the removal of licenses, if not corrected.
Fines should be applied on a ‘results basis’ as opposed to a ‘behavioural basis’ to prevent dishonest actors from avoiding responsibility by claiming accidental incompetence.
To clarify: this paper focuses mainly on visa overstays. The issue of asylum claimants via the Channel crossings is not touched on. A paper will follow in due course, addressing the abuse of the European Convention on Human Rights (Article 8) and its incorporation into UK law (Human Rights Act, 1998).
Fixing Healthcare and Illegal Immigration
Highlighting the use of our health services by unauthorised migrants is just the first step. We include this last section to counter narratives that addressing illegal migration is logistically insurmountable. To date, across the spectrum, Nigel Farage has touched on some of the logistical challenges (GB News), whilst Jeremy Hunt has tried to outline a ‘multi-front’ approach (Daily T, Telegraph podcast).
It is not good enough that successive Labour and Tory Governments would rather absorb excess visa overstayers into the health system (and generally across the country) than effectively deport illegal immigrants.
We assess that without having to set up charter flights or new deportation centres, the UK’s current commercial flight capacity could support deportations for visa overstayers and lighten the long-term burden on our health system.
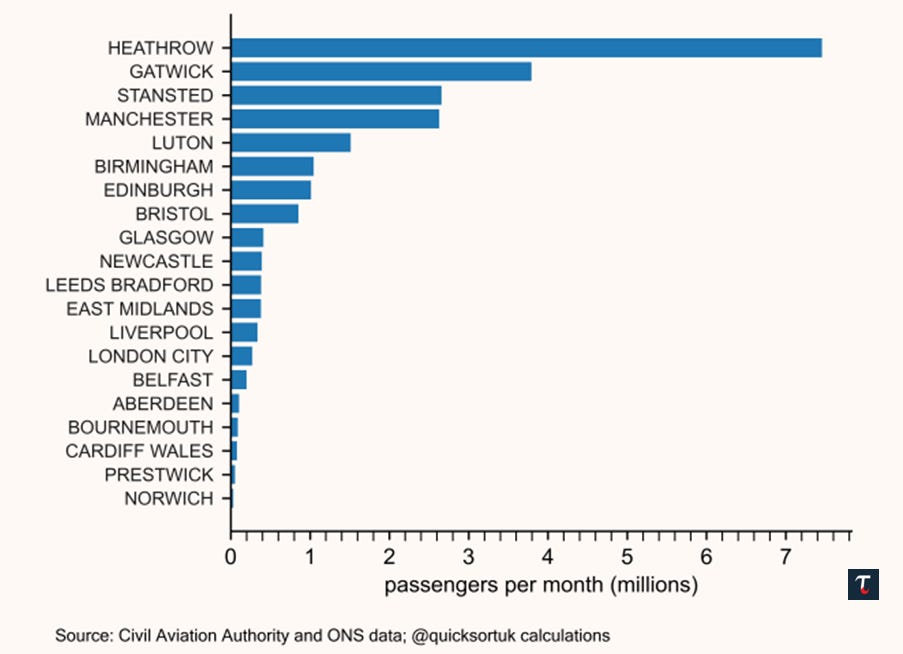
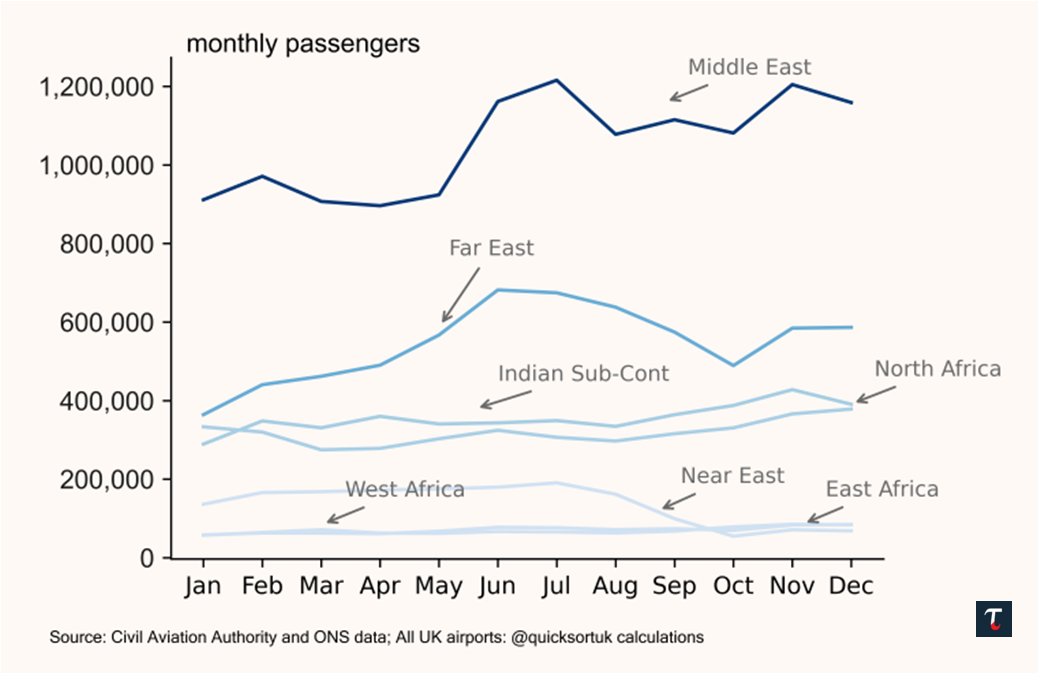
Heathrow alone handles around 7 million passengers (see Exhibit 8), while the UK’s total passenger traffic to and from North Africa routinely flies 300,000 passengers a month (see Exhibit 9). Assigning a handful of seats per flight on these routes (with an appropriate surcharge) would quickly enable tens of thousands of visa overstay deportations.
This could be easily leveraged and paid for by the home countries of these visa overstayers. Non-cooperation by either individuals or their home countries could result in visa caps or suspensions, visa or flight surcharges, remittance taxes, and economic sanctions.
The visa overstay angle is —in many ways— less immediately challenging than dealing with traditional asylum claimants. Many of them (by definition) do not have credible grounds to retrospectively claim asylum, and have simply been exploiting a failed British immigration system for years.
Any policy must operate from first principles. The incentives must ensure that the optimal thing for an illegal worker is to leave voluntarily. Illegal migrants should conclude it is better to leave early and quickly than suffer consequences back home, if an expensive forced deportation were to take place. Equally, while there should be penalties for the support network (be it one’s employer or relatives), there should be an option to report. self-report without penalty, or even a modest financial reward — as an off-ramp.
With 43% of day-to-day fiscal spending (2025) going towards health and a whole assortment of real economic challenges facing Britain, we must end the permissive attitudes in our current immigration system.78 We hope this paper spurs practical action to address illegal immigration, particularly visa overstays, and the rise in NHS GP patient registrations.
If you enjoyed this Report, feel free to like and share. For further work on this, and other subjects, follow Trafalgar Analytics on Twitter / Substack.
—
@quicksortuk, @jessgill03 and @Eulipotyphla_OG,
Trafalgar Analytics, 3rd July 2025.
The authors would like to thank @AylmerTH for assisting the raw data compilation.
Trafalgar Analytics is Britain’s pioneering data analytics and research unit. We focus on the discovery, interpretation, and communication of meaningful patterns in data. We believe in a data driven approach to tackling the foremost societal, economic, and political challenges of our time.
If you are interested in supporting, collaborating, or working with us, do not hesitate to get in touch: trafalgaranalytics@protonmail.com
References and Footnotes
NHS (2023). How to register with a GP surgery. [online] nhs.uk. Available at: https://www.nhs.uk/nhs-services/gps/how-to-register-with-a-gp-surgery/.
Cuibus, M. V., & Walsh, P. W. (2025) Unauthorised migration in the UK. Migration Observatory briefing, COMPAS, University of Oxford. Available at: https://migrationobservatory.ox.ac.uk/resources/briefings/unauthorised-migration-in-the-uk/.
Lindrop, J. (2019). Measuring illegal migration: our current view. [online] Office for National Statistics. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/internationalmigration/articles/measuringillegalmigrationourcurrentview/2019-06-21.
Home Office (2022). Developments in Exit Checks. [online] GOV.uk. Available at: https://www.gov.uk/government/statistics/developments-in-exit-checks/developments-in-exit-checks.
Churchill Healthcare (2025). Safe Surgeries New Patient Registration Policy. [online] Churchill Medical Centre. Available at: https://www.churchillmedical.nhs.uk/policies/safe-surgeries-new-patient-registration-policy/.
O’Brien, N. (2024). Changing HIV strategy. [online] Neilobrien.co.uk. Available at: https://www.neilobrien.co.uk/p/changing-hiv-strategy.
Triggle, N. (2024). Health spending £5bn less than government planned. BBC News. [online] 14 May. Available at: https://www.bbc.co.uk/news/health-69005259.
Note: Day-to-day fiscal (government) spending, excludes capital investments in long term assets.
What a very impressive piece. Very well written and impeccably researched. Thank you very much.
Shocking.